If you or a loved one are facing a diagnosis of aplastic anemia, one of the first and most frightening questions is often, “How long can you live with this?” It's a valid concern. Aplastic anemia is a rare but serious blood disorder in which bone marrow fails to produce enough blood cells, leaving the body vulnerable to fatigue, infection, and bleeding. The good news? Treatment options have improved dramatically. A recent report suggested very high post-transplant survival especially in younger patientsand large registry studies now show 5-year survival rates of around 64–77% after hematopoietic stem cell transplant, depending on age and donor match. Importantly, patients who make it through the first year of treatment often go on to have a long-term life expectancy almost comparable to the general population. In this guide, we’ll walk you through what exactly aplastic anemia is, how to spot the warning signs, what causes it, and the modern treatment approaches that offer real, evidence-based hope.
.jpg "Aplastic Anemia: Warning Signs, Causes & Modern Treatments (2025)")
Understanding Aplastic Anemia
What Is Aplastic Anemia?
Aplastic anemia is a rare blood disorder that occurs when your bone marrow the spongy material inside your bones—cannot produce enough new blood cells . It's fundamentally a form of bone marrow failure. Unlike some other types of anemia that involve a lack of specific nutrients, the problem in aplastic anemia lies in the factory itself. The hematopoietic stem cells in your marrow are damaged, leading to a shutdown in the production of red blood cells, white blood cells, and platelets . This results in a condition known as pancytopenia, which means you have low counts of all three blood cell types .
Types of Anemia Including Aplastic Anemia
To understand what makes aplastic anemia unique, it helps to know about the broader landscape of anemic conditions.
What Are the Five Main Types of Anemia?
While there are many specific types, they often fall into these five broad categories based on their cause:
Iron-deficiency anemia: The most common type worldwide, caused by a lack of iron, which is essential for making hemoglobin .
Vitamin-deficiency anemia: Caused by low levels of vitamin B12 or folate (folic acid), which are also crucial for red blood cell production .
Hemolytic anemia: Occurs when red blood cells are destroyed faster than the bone marrow can replace them .
Sickle cell anemia: An inherited form of hemolytic anemia where a genetic defect causes red blood cells to become misshapen (sickle-shaped), rigid, and prone to breaking apart .
Aplastic anemia: Caused by bone marrow failure, leading to a failure to produce all types of blood cells .
How Is Aplastic Anemia Different from Other Types?
The key difference is the scope and nature of the problem. Most anemias, like iron deficiency or sickle cell, primarily affect red blood cells. Aplastic anemia is distinct because it causes a pancytopenia a shortage of all blood cells (red cells, white cells, and platelets).
This means the consequences are broader: you don't just experience fatigue from anemia, but also have a dramatically increased risk of infections from low white blood cells (neutropenia) and a higher risk of bleeding or bruising from low platelets (thrombocytopenia) . It's not a problem with the quality or components of the blood cells (like in sickle cell) or a lack of building blocks (like iron), but with the blood cell factory itself shutting down.
Causes of Aplastic Anemia
What Is the Most Common Cause of Aplastic Anemia?
In the majority of cases, the precise trigger is unknown, a situation referred to as idiopathic aplastic anemia . However, researchers believe that the most common underlying mechanism is an autoimmune bone marrow damage . This means the body's own immune system mistakenly attacks and destroys the hematopoietic stem cells in the bone marrow, shutting down blood cell production .
Common Causes: Drugs, Chemicals, Viruses
A range of external factors can injure the bone marrow or trigger the autoimmune response:
Chemical Exposure: Exposure to toxic chemicals, such as benzene (found in gasoline and used in some industries), pesticides, and insecticides, has been linked to the disease .
Drugs: Certain prescription medications, including some antibiotics and drugs used for rheumatoid arthritis, have been associated with aplastic anemia .
Viral Infection: Viruses like Epstein-Barr (EBV), cytomegalovirus (CMV), HIV, and hepatitis have been known to play a role in triggering the disorder . In some cases, aplastic anemia can follow an episode of seronegative hepatitis .
Immune System and Bone Marrow Damage
As an autoimmune disorder, aplastic anemia is driven by T-cells that attack the bone marrow. These immune cells release cytokines that damage stem cells and disrupt the blood-forming process . This understanding is why immunosuppressive therapy, which calms this misguided immune attack, is a cornerstone of treatment.
Genetic and Inherited Factors
While most cases are acquired after birth, aplastic anemia can also be part of rare inherited aplastic anemia syndromes. The most common of these is Fanconi anemia . Other inherited bone marrow failure syndromes include dyskeratosis congenita and Shwachman-Diamond syndrome . These are typically diagnosed in childhood and are associated with other physical abnormalities.
How Serious Is Aplastic Anemia?
Aplastic anemia is a life-threatening condition if left untreated . Its severity is classified based on blood cell counts:
Non-Severe (NSAA): Milder form.
Severe (SAA): Defined by very low neutrophil and platelet counts .
Very Severe (VSAA): The most critical form, with an extremely low neutrophil count .
The seriousness stems from the risk of uncontrollable bleeding, severe infections, and heart complications from profound anemia . However, with modern treatment, the prognosis has improved dramatically.
Symptoms and Early Warning Signs
What Are Common Early Signs of Aplastic Anemia?
Here's a crucial point that can sometimes cause delay in diagnosis Aplastic anemia can have no symptoms in its earliest stages. When the blood cell counts are only slightly low, you might not feel anything wrong. However, as the bone marrow failure becomes more severe and blood cell counts drop, symptoms will begin to appear.
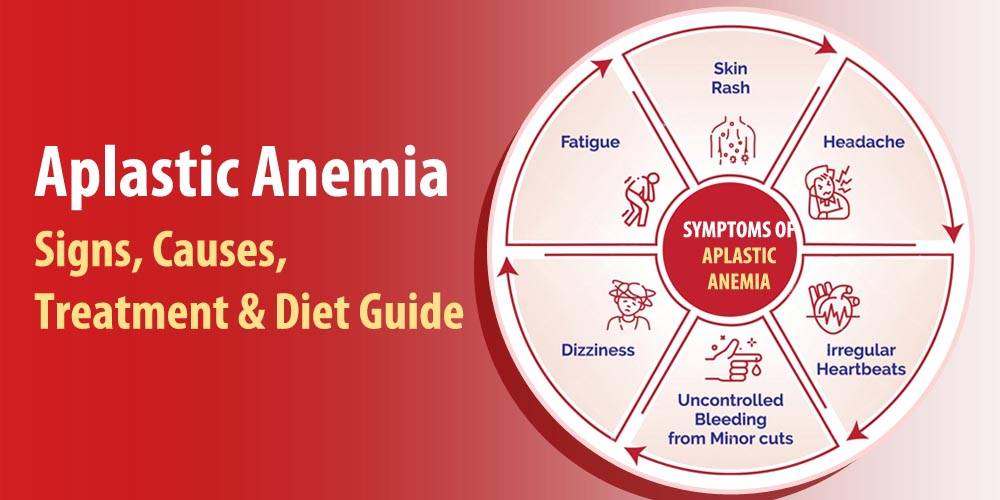
The signs are directly tied to the shortages of specific blood cells, a condition known as pancytopenia. Here’s what to look out for:
Fatigue and Shortness of Breath: This isn't just ordinary tiredness; it's a profound and persistent exhaustion caused by a severe lack of red blood cells (anemia). You might feel dizzy, weak, or get short of breath even after minor activities like walking across a room.
Rapid or Irregular Heart Rate (Palpitations): Your heart has to work much harder to pump the limited oxygen in your blood throughout your body. This can cause a feeling that your heart is racing, pounding, or fluttering.
Frequent or Prolonged Infections: With a critically low number of infection-fighting white blood cells (neutropenia), your body can't defend itself. You may find you catch every bug that goes around, infections last longer, and you might experience recurrent fevers without an obvious cause.
Unexplained or Easy Bruising: A slight bump might cause a large, dark bruise. This happens due to a very low platelet count (thrombocytopenia), which means your blood has trouble clotting.
Bleeding Episodes: This includes frequent nosebleeds, bleeding from the gums after brushing your teeth, and prolonged bleeding from minor cuts that would normally stop quickly.
Pale Skin: A pale complexion, often with a whitish tint to the mucous membranes inside the mouth and lower eyelids, is a classic sign of anemia.
Skin Rash: The rash associated with aplastic anemia isn't itchy like an allergy. It's often a sign of bleeding under the skin. You might notice petechiae (tiny, pinprick red or purple spots) or larger purplish patches called purpura, both caused by minor capillary bleeding due to low platelets.
Fever: A persistent or recurring fever is a common sign of an underlying infection that your body is struggling to fight off.
How Does Aplastic Anemia Affect the Body?
The symptoms listed above show how aplastic anemia is a systemic disease. It doesn't just affect one part of you. The lack of red blood cells starves your tissues of oxygen, the lack of white blood cells leaves you defenseless, and the lack of platelets prevents you from stopping bleeding. It's a triple threat that impacts your energy, your immune system, and your body's basic repair mechanisms.
Can Anemia Cause Tingling or Rash?
As we've covered, a rash is indeed a common sign, but it's specific in its nature it's a bleeding rash, not an allergic one. Tingling in the hands and feet (paresthesia), however, is not a typical symptom of aplastic anemia. This sensation is far more characteristic of anemias caused by a vitamin B12 deficiency (pernicious anemia), which can damage nerves. If you are experiencing tingling, it's important to tell your doctor, as it helps them distinguish between different types of anemia.
Diagnosis of Aplastic Anemia
Blood Tests and Pancytopenia
The first step in diagnosis is usually a complete blood count (CBC). The hallmark finding is pancytopenia low counts of red cells, white cells, and platelets. A low reticulocyte count (immature red blood cells) is also a key indicator, as it shows the bone marrow is not producing new cells effectively .
Bone Marrow Biopsy and Stem Cell Analysis
A bone marrow biopsy is essential to confirm the diagnosis. During this procedure, a small sample of bone marrow is taken, usually from the hip bone. In aplastic anemia, the marrow will be hypocellular meaning it is abnormally fatty and empty, with a marked absence of blood-forming cells . This test helps rule out other diseases like leukemia or myelodysplastic syndromes (MDS), where the marrow is often crowded with abnormal cells .
Treatment and Prognosis
Can Aplastic Anemia Be Cured?
Yes, aplastic anemia can be cured. The only definitive cure is an allogeneic stem cell transplant (also called a bone marrow transplant) . For those who are not candidates for a transplant, immunosuppressive therapy (IST) can induce long-term remission, allowing many patients to live normal lives, though it may not be considered a permanent cure .
The following table summarizes the main treatment options and their goals:
|
Treatment Option |
How It Works |
Key Considerations |
|
Stem Cell Transplant |
Replaces damaged bone marrow with healthy stem cells from a donor. |
The only potential cure. Success is highest in younger patients with a matched donor . |
|
Immunosuppressive Therapy (IST) |
Uses drugs to stop the immune system from attacking the bone marrow. |
A combination of anti-thymocyte globulin (ATG) and cyclosporine is standard . |
|
Blood Transfusion |
Replaces red blood cells and platelets to relieve symptoms. |
Supportive care, not a treatment for the disease itself. Manages symptoms and prevents complications . |
Immunosuppressive Therapy and Drugs
This is often the first-line treatment for many adults and those without a matched donor. It typically involves a combination of:
Anti-thymocyte globulin (ATG): A powerful antibody that suppresses the immune system's T-cells .
Cyclosporine: An oral immunosuppressant that helps prevent the immune system from attacking the marrow .
This combination therapy aims to allow the bone marrow to recover and resume normal blood cell production.
Managing Side Effects and Complications
Treatments come with potential side effects. Immunosuppressants increase infection risk, and transplants carry a risk of graft-versus-host disease . Blood transfusions can lead to iron overload, which requires additional management. A dedicated medical team is essential to monitor and manage these complications.
Living with Aplastic Anemia
Can You Live a Full Life With Aplastic Anemia?
Absolutely. Many people with aplastic anemia, especially those who respond well to treatment, can live full, productive lives . The key is consistent follow-up care to monitor blood counts, manage treatment side effects, and watch for any signs of relapse or, rarely, evolution into another blood disorder.
Special Considerations: Pregnancy and Quality of Life
Pregnancy can pose a significant risk for women with aplastic anemia, as it can worsen the condition and poses risks to both mother and baby . Care from a high-risk obstetrician and a hematologist is essential. For quality of life, patients are advised to:
Avoid high-contact sports to prevent bleeding .
Practice meticulous hygiene to prevent infections .
Ensure adequate rest to combat fatigue.
Recommended Diet, Food, Exercise for Aplastic Anemia Patient
While diet cannot cure aplastic anemia, good nutrition supports overall health during treatment.
Diet: Focus on a balanced diet. Because of infection risk, you may be advised to avoid raw or undercooked foods, unwashed fruits and vegetables, and unpasteurized products.
Food: No specific food will reverse bone marrow failure, but eating iron-rich foods (like lean meats and leafy greens) and vitamin-rich foods is generally recommended for overall well-being .
Exercise: Gentle exercise like walking can help with stress and fatigue, but it's crucial to consult your doctor before starting any new routine, especially with a low platelet count .
When to know require medical support
Receiving an aplastic anemia diagnosis can be overwhelming. However, it's important to focus on the facts this is a treatable disease. Modern medicine offers powerful options, from potentially curative transplants to highly effective immunosuppressive therapies that can induce long-term remission. The survival rates, particularly for younger patients, are more promising than ever. If you recognize the warning signs or symptoms unexplained fatigue, frequent infections, or easy bruising the most critical step is to seek medical evaluation. With an early diagnosis and a dedicated healthcare team, you can navigate this challenge and move forward with hope.
Frequently Asked Questions (FAQ)
What Is the Survival Rate of Aplastic Anemia?
Survival rates have improved dramatically and depend heavily on age and treatment. A large Swedish study found the 5-year survival rate to be over 90% for patients aged 0-39 years. For those aged 40-59, it was 70.7%, and for patients 60 and over, it was 38.1%, highlighting the challenge of managing the disease in older adults . With a stem cell transplant, one center reported a 96% overall survival rate .
Is Aplastic Anemia a Terminal Illness?
No, aplastic anemia is not necessarily a terminal illness. While it is a serious and life-threatening condition if left untreated, it is now considered a highly treatable disease for most patients. With modern therapies like immunosuppression and stem cell transplantation, the vast majority of patients, especially younger ones, can achieve long-term survival and remission .
Can Bone Marrow Regenerate Itself?
In aplastic anemia, the bone marrow's ability to regenerate is suppressed, primarily by the immune system. The goal of treatment is to remove that suppression (through immunosuppressive therapy) or replace the faulty marrow entirely (through transplant). When this is achieved, the bone marrow can often recover and resume normal blood cell production .
What Should You Avoid If You Have Anemia?
If you have aplastic anemia, you should take precautions to prevent bleeding and infection:
Avoid high-contact sports like football or hockey .
Avoid medications that can increase bleeding risk, such as aspirin and ibuprofen, unless approved by your doctor.
Avoid exposure to people who are sick to reduce infection risk.
Avoid activities that could cause injury or bruising.
What Are the Main Causes of Anemia?
Anemia has many causes, which is why a proper diagnosis is key. The main causes include :
Blood loss (e.g., from heavy periods or a stomach ulcer).
Lack of iron, vitamin B12, or folate in the diet.
Chronic diseases (e.g., kidney disease, cancer).
Inherited conditions (e.g., sickle cell anemia, thalassemia).
Bone marrow problems, such as aplastic anemia or leukemia.
Important Medical Disclaimer: This content is based on current medical literature but is not a replacement for personalized medical care. The treatments and outcomes mentioned are general and may not apply to your specific situation. We strongly advise you to consult with a qualified hematologist or your primary care doctor for an accurate diagnosis and a treatment plan tailored to your health needs.